Enquiry Stage 2: Advice for Conducting an Adult Safeguarding Enquiry
1. The decision-making process
The Multi-Agency Adult Safeguarding Concern Form has been designed to provide all of the detailed and necessary information to allow colleagues in the Local Authority to effectively make a decision on if a Safeguarding Concern needs to progress to a Section 42 (or Other Enquiry) under the Local Authorities duty to do so within the Care Act 2014.
Please also refer to: Guidance for Making Decisions on Adult Safeguarding Enquiries
All of this Safeguarding data will be collated within the Local Authorities case management system (as the lead agency in the Borough) so that there is a central source of information and intelligence, which will allow this to be carefully monitored and assessed.
Also carefully consider if statutory advocacy is required: Advocacy 7 Minute Briefing March 2023
2. Enquiry routes
Once a decision is made that a Safeguarding Enquiry must be conducted under the Section 42 duty, the relevant team within the Local Authority will decide who is best placed to conduct this, directing it through one of the four strands (2.1 to 2.4) outlined below. When this is delegated outside of the Local Authority they will still retain the overall responsibility to co-ordinate the enquiry as the lead agency, and as such they will provide the quality assurance and oversight in relation to all Safeguarding Enquiries.
S42 Enquiry Report Template (Pdf) S42 Enquiry Report Template (Word Version)
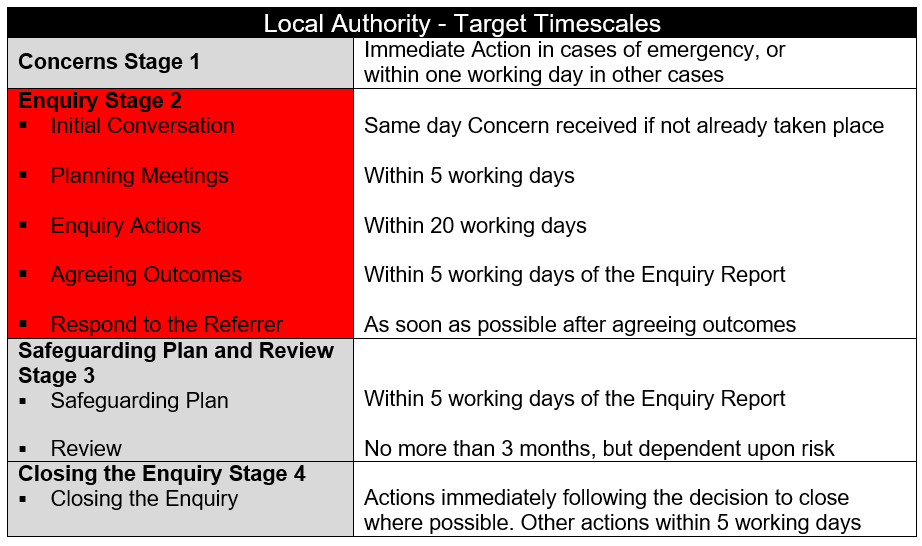
Professionals should also read the London Multi-Agency Safeguarding Policy and Procedures (pages 66-78) for further information on conducting Adult Safeguarding Enquiries, using the checklists and detailed good practice guidance (target timescales are the bottom of this page).
2.1 Police investigation
If a Safeguarding Concern has been submitted to the Local Authority and it is identified that an element, or all of this Concern may be linked to criminal activity, then the early involvement of police is essential. Police investigations should be coordinated by the local police MaSH team who may also support other parallel actions or enquiry options, but this should always be police led.
See pages 67-68 of the London Multi-Agency Safeguarding Policy and Procedures for more information.
2.2 Standard delegation within the London Borough of Lewisham (LBL) Council
All social work staff within LBL can have Safeguarding Enquiries delegated to them, normally through one of the following four main strands:
- Neighbourhood Teams 1-4 (London Borough of Lewisham).
- Placements Team (London Borough of Lewisham).
- Hospital Social Work Team (University Hospital Lewisham).
- Mental Health Social Work Teams within South London and Maudsley (SLaM) NHS Foundation Trust.
There is a need for supervision and co-ordination of enquiries by Safeguarding Adults Managers (SAMs).
See pages 57-58 of the London Multi-Agency Safeguarding Policy and Procedures for more information.
2.3 External delegation
Safeguarding Enquiries or elements of them may also be routinely delegated outside of LBL to the following partners:
- Lewisham and Greenwich NHS Trust (LGT) Safeguarding Team, who may then sub-delegate across their internal divisions, including to the District Nursing Service.
- South London and Maudsley NHS Foundation Trust (SLaM).
- South East London (SEL) Integrated Care Board (ICB).
- Care and Nursing Homes.
- Home Care Providers.
- GP Practices.
- Other Service Providers.
Causing S.42 Enquiries Letter Template (Word)
SAMs will also need to supervise and co-ordinate these enquiries.
2.4 Referrals to Pressure Ulcer Panels (PUPs)
Potential Safeguarding Concerns linked to pressure ulcers can be challenging as it needs to be determined if this has been caused by poor quality care or evidence of neglect or omissions in care provision. This can occur due to other associated factors and may require input from a professional for clinical judgements to be considered:
The person’s physical and mental health.
- Multiple co-morbidities.
- State of overall skin condition of the person.
- Indicators of neglect of care provision in relation to hygiene and/or repositioning.
- Evidence of ineffective continence management.
- Evidence of ineffective nutritional and fluid management.
- Ineffective Pain management.
- Evidence of completed and accurate proactive risk and wound assessments and subsequent care planning.
- Accurate monitoring and recording in all documentation.
- The views of the service user, family and friends on treatment and care are recorded.
- Capacity and level of engagement of service users and others.
- Evidence of appropriate and timely referrals to members of multidisciplinary team.
- Views of others including professionals.
Pressure Ulcer Panel Process - University Hospital Lewisham Dec 2020
Pressure Ulcer Panel Process - In the Community Sept 2022
While Pressure Ulcers are a risk for people who are frail and not able to move easily, with good management and care these can be prevented. If an adult at risk has a pressure ulcer this should not been as a reason to automatically suspect abuse or neglect, although this should be carefully considered, and a Safeguarding Concern must always be submitted for a stage 3, 4, Unstageable, Deep Tissue Injury and Medical Device pressure ulcers.
If a Safeguarding Concern has been submitted for a pressure ulcer related matter the Local Authority will pass this case onto the relevant Pressure Ulcer Panel (PUP) to oversee the initial investigation:
- The Community PUP - overseen by the South East London, Integrated Care Board. (Care Home Only).
- The Acute Trust’s PUP - overseen by Lewisham and Greenwich NHS Trust. (Trust Acute and Community Service).
Health professionals will then inform the safeguarding process by conducting a Pressure Ulcer Synopsis and Root Cause Analysis (RCA) and submit the relevant reports to the appropriate PUP. The Lewisham Multi-Agency Safeguarding Hub (MaSH) will provide the initial support and oversight of pressure ulcer related cases until the RCA has been completed.
If the pressure ulcer amounts to the wilful neglect of an individual who lacks mental capacity, a crime under section 44 of the Mental Capacity Act 2005 may have occurred, and in these instances the police will be informed.
SAM’s should engage with the PUP’s to gain understanding of process and decision making of PUP professionals, alongside assisting to co-ordinate any other elements of the safeguarding enquiry if there is another aspect to this.
The PUP’s will attempt to conclude their investigation within 28 days, but this may not always be possible. Once the PUP’s have decided no further investigation by panel is required, the enquiry is closed to the panel and an action plan process is implemented. The SAM should then co-ordinate any further actions up to the point of the enquiry being closed overall.
3. Consent and engagement with the adult in relation to a Safeguarding Enquiry
These are often crucial factors in determining if a Safeguarding Enquiry can progress, and how effective it is, and may lead to decisions not to proceed that leave the adult still exposed to a risk of significant harm.
- Read The Caldicott Principles.
- Also see Information Sharing page which is full of advice, guidance and the local Information Sharing Agreement.
- Does the adult have the mental capacity to consent to the Safeguarding Enquiry?
- Is there a need to provide statutory advocacy: Advocacy 7 Minute Briefing March 2023
- Is there any possibility that the adult has/ is suffering from any type of coercion, control, threat, duress or pressure from another person(s) which may mean they refuse consent?
- Does mental capacity (including executive capacity) need to be assessed or reviewed? For more information read: Decision Making and Mental Capacity (NICE Guidelines), Supported decision-making toolkit for people with communication difficulties Practicable steps for people with communication difficulties and Oldham SAB's Executive Functioning Guidance
- Give due regard to the adult’s views and wishes, including their desired outcomes, even if Best Interest Decisions have been made linked to the Mental Capacity Act. For more information read: Local Government Association - Making Safeguarding Personal Toolkit including on the six Safeguarding Principles and Alcohol Change UK Cognitive Impairment Guide and Alcohol Change UK How to use legal powers to safeguard highly vulnerable dependent drinkers guide.
- If the adult does have the mental capacity to consent to the Safeguarding Enquiry, but refuses, professionals must be careful that they consider how to keep the adult safe. This may be particularly relevant in domestic abuse cases.
- A Safeguarding Enquiry can still proceed without the adult’s consent if ‘vital’ or ‘public’ interest considerations apply.
- If the adult meets the safeguarding duty/ criteria, and is at risk of significant harm, and it is deemed they do have the mental capacity to refuse consent and to not engage with any Safeguarding Enquiry, then consider seeking legal advice and the use of the Court of Protection, and or Inherent Jurisdiction: 39 Essex Chambers: Guidance on Use of Inherent Jurisdiction.
- See and use the Guidance on Improving our Approach to Adult and Family Engagement which includes an overview of Trauma Informed Practice.
- See and use the Multi-Agency Self-Neglect Policy, Practice Guidance and Procedures.
- Professionals must consider escalating decision making where necessary in more complex cases, and respectfully challenge decision making if necessary and appropriate Inter-Agency Escalation Policy July 2023
- This links to the subject of Professional Curiosity as it is good practice to respectfully challenge safeguarding decisions that you believe are not appropriate. Please Read This Guidance: Lewisham Safeguarding Adults Board - Professional Curiosity
4. The Challenge of Engagement and Self-Neglect
Only 5% of Section 42 Enquiries are related to Self-Neglect in Lewisham, but professionals must understand the significance of these complex cases as almost half of all Safeguarding Adults Reviews, and therefore some of the most serious cases of abuse nationally, are related to this subject.
When an adult is self-neglecting, relationship based work becomes crucial and having one worker as a single point of contact may be beneficial.
Using the label “hard to engage” is damaging and may result in other professionals believing there is little point in attempting to do so, and therefore should be avoided (“seldom heard” may be a more appropriate term).
Practitioners should work together if one is struggling to achieve meaningful engagement with the adult, as another may still be able to take the lead on behalf of an Enquiry Officer in managing and monitoring risk.
Practitioners should also consider the following in helping to improve engagement with adults:
- Creative, flexible and imaginative ways to communicate with adults, including working with faith, community leaders and non-safeguarding practitioners to achieve the best outcomes.
- Producing information in a number of ways to meet individual needs.
- Involving family members appropriately to help support adults.
- The use of advocacy to engage with adults.
- Training staff to enable and improve engagement with adults.
Multi-Agency Self Neglect Policy, Practice Guidance and Procedures
5. Making Safeguarding Personal during a Safeguarding Enquiry
Making Safeguarding Personal (MSP) is an initiative which aims to develop a person centred and outcomes focus to safeguarding work in supporting people to improve or resolve their circumstances.
What MSP Seeks to achieve:
- A personalised approach enabling safeguarding to be done with and not to people, using practical methods defined by the adults individual needs rather than those of the organisation.
- The outcomes an adult wants, by determining these at the beginning of working with them, and ascertaining if those outcomes were realised at the end.
- Improvement to people’s circumstances rather than on ‘investigation and conclusion’.
- Utilisation of person-centred practice rather than ‘putting people through a process’.
- Good outcomes for people by working with them in a timely way, rather than one constrained by timescales.
- Improved practice by supporting a range of methods for staff learning and development.
- Learning through sharing good practice.
- Further development of recording systems in order to understand what works well.
- Broader cultural change and commitment within organisations, to enable practitioners, families, teams and the Lewisham Safeguarding Adults Board to know what difference has been made.
Supporting people living with Dementia to be involved in adult Safeguarding Enquiries (March 2021)
Making Safeguarding Personal | Local Government Association
……………………………………………………………………………………………………………………………………………
Safeguarding Principle - Empowerment
What does this mean for the professionals: Adults are encouraged to make their own decisions and are provided with support and information.
What does this mean for the adult: "I am consulted about the outcomes I want from the safeguarding process and these directly inform what happens". ……………………………………………………………………………………………………………………………………………
Local Government Association - Making Safeguarding Personal Toolkit